 By Elizabeth Payne Leaving the NICU with your baby is exciting and nerve wracking all at the same time. Although this is a time to celebrate- your baby is healthy enough to go home with you!- many parents are scared by the fact that they are moving baby from an environment where they are constantly surrounded by doctors and nurses to one where they usually have only two people watching them. Your baby’s care team will help you make the transition from hospital to home, but the following guide will give you a good general idea of what to expect, as well as suggestions to help ease you into the transition. Preparing to Go Home If your baby was born prematurely, there are several requirements they must meet to be eligible to go home; they must be gaining weight steadily, be able to maintain their body temperature, and no longer require tube feedings; some wards will also require a minimum weight. Most children reach these milestones around their original due date, but this is not a hard and fast rule. Each baby varies and your particular child may be discharged up to a month in advance of this date, or several weeks after. Prior to discharge, your medical care team will come up with a care plan for you and your child, which will detail the special needs your child may have and how to help with them. They will also help you determine your child’s nutritional needs, sleep, eating and medicine schedules and everything else you need to know. Remember, if you’re confused about something or want to know more about it, ask. If your baby requires the use of medical devices at home, the medical team will train you in the use of them before you go home. You may also be trained in infant CPR if your baby has certain breathing problems; if this is necessary, your baby should always have someone trained in infant CPR with them. This means that all caretakers; you, you partner, aunts, uncles, grandparents, family friends, or anyone else who will be alone with the baby for any period of time, should be trained in how and when to perform infant CPR. The medical team will also tell you if you should be on the lookout for any particular behaviors and to react to the. Remember that you can call your doctor any time after discharge if you have any additional questions. Before leaving the hospital, you should pick a pediatrician for your child and meet with them. It is good to establish a relationship with your child’s doctor early on and inform them of any special care they may require. The first appointment with the pediatrician should take place within a few days of discharge. Before leaving, ensure that you have all the paperwork pertaining to your baby’s health in order, preferably in its own file; medication sheets, test results, personal notes, discharge summaries, and names and numbers of doctors and specialists. Keeping this all together now will save you later when you need it.   Help at Home It takes a village to raise a child, and NICU babies are no exception to this. Reaching out for help from family, friends and professionals will benefit you greatly, especially during the stressful first few days at home. Some insurance companies cover the costs of a visiting nurse for new parents, which many parents find great comfort in. Visiting nurses allow you to increase your confidence in caring for your child at home, while also providing a “safety net” and assurance that you’re doing the right thing. However, even if your insurance doesn’t cover this, early intervention programs for NICU graduates will often provide free home visits that will provide you with the same level of comfort (see the early intervention section below for more details). Family and friends are also a great resource during this time. Don’t be afraid to reach out for or accept help. The people who love you understand that you still need help, and there is no shame in respectfully asking them to pick up something from the pharmacy, assist with meal preparation, or help with the household tasks you’ve fallen behind on. This is especially true if you have other children, who are probably feeling ignored in favor of their new sibling; getting help can give you more time to spend with the older kids, or will let you send them out of the house for a playdate and make them feel appreciated while you dote on baby. Early Intervention Programs Early intervention, or EI, programs are designed to help children who have or are at risk for developmental delays. This includes almost all NICU graduates. Your child will be evaluated, and if they meet the criteria, will be referred to an early intervention program. Remember that there is no shame in this and this in no way reflects on you. Your baby just made it through a very tough stay in the NICU and might need a bit more help in the beginning of their life. EI programs can provide myriad free services to your family that can help ease you and baby into life after the NICU, such as home visits, counseling, therapy, support groups, education, and nursing and nutritional services. Visitors Staying cooped up at home without any visitors constantly is stressful for both you and your child. However, you will probably be nervous about taking your little NICU graduate out or having visitors over, and rightly so. Prior to hosting visitors, make sure to lay some ground rules with them, such as washing hands before visiting and again prior to holding the baby, no visits if you’re sick, and that anyone who smokes should shower and change their clothes before coming over. You should emphasize how important it is to keep your home disease free for the safety of your newborn; freely remind visitors that an adult’s little cold can be a big threat to your child, and suggest that school age children and anyone who has a sick person in their household hold off on visits for a while. Also, it is okay to gently remind your guests that your baby is on a schedule and you may need to excuse yourself to pump or feed, or possibly shoo everyone from the room when nap time rolls around. Remind them that although they may want to spend time with the baby, your child’s health is paramount and you little one needs a quiet, clean environment. If your child is seriously immunocompromised, you may be put on quarantine until their system is healthy enough to handle everyday germs. Although this is the best option for your child’s physical health, this might take a toll on your mental health. Just because you are stuck in the house without visitors doesn’t mean you have to be lonely; try to keep in touch with friends through social media, phone calls, e-mails, anything you can think of. Encourage them to contact you and update you on their lives and share news about your family with them. When to Call the Doctor It is better safe than sorry. If you think that there is something wrong or have a question, call your doctor. There are many other resources available for you to use, but most of them don’t have a medical degree and don’t know your baby. You should additionally, with no second thought, call your child’s doctor if you notice that your child has yellowed skin or eyes, has a temperature of over 100 degrees F, has breathing trouble, is difficult to wake up, has blood in their vomit or diaper, or has a seizure. Sources: http://kidshealth.org/parent/pregnancy_center/newborn_care/preemie_home.html# http://www.ahrq.gov/professionals/systems/hospital/nicu_toolkit/nicupacket.pdf http://www.marchofdimes.org/baby/getting-services-for-your-baby-after-the-nicu.aspx http://www.babyfirst.com/en/parents-corner/life-after-neonatal-intensive-care-unit.php http://handtohold.org/resources/helpful-articles/coming-home-from-the-nicu/  By: Elizabeth Payne It is hard to believe that only a century ago, most sickly and premature infants were sent home from the hospital without any special interventions; many of these children did not survive past their first birthday. The first neonatal intensive care units did not even appear in American hospitals until 1922; however, special care methods for infants began to be developed in the late nineteenth century. The Pre-NICU Era (up to the 1950's) Pierre-Constant Budin (November 9, 1846 – January 22, 1907) Pierre-Constant Budin (November 9, 1846 – January 22, 1907) Pierre-Constant Budin, a French obstetrician, was a pioneer in the care of at risk babies and devoted his career to reducing infant mortality. He encouraged educating new mothers about proper nutrition and hygiene for their babies, and knowing the risks contaminated cow’s milk could pose to newborns, urged the use of breast milk instead of cow’s milk, and believed that sterilized cow’s milk should be used if breast milk was insufficient. He also brought gavage- the process of feeding through a tube that went directly to the stomach- into the spotlight, helping premature infants who were unable to feed normally receive the nutrition they needed. Budin started his career as an assistant to Etienne Stephane Tarnier, another French obstetrician instrumental in the development for neonatal care. Infants that are born too early are often incapable of producing their own heat, and incubators help keep these babies warm and allow them to use their energy to grow and gain weight. Tarnier recognized this, and developed a crude isolette- a wooden box with a glass lid and a hot water bottle inside- to put premature infants inside of. Tarnier’s work contributed to a 28% decrease in infant mortality over three years at the French maternity hospital he worked in. Tarnier’s technology was picked up by a student of Budin’s, Martin Couney, who used considerably less conventional methods to help popularize special care for premature infants outside of France. 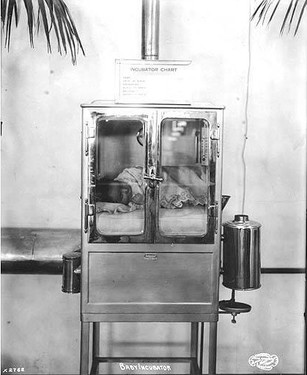 At the turn of the century, many hospitals in both America and Europe did not allow technology such as incubators to be used within their walls. Couney, however, recognized the potential of incubators for helping premature babies. Dr. Couney offered this type of treatment for premature infants free of charge; it was paid for through admissions. Dr. Couney displayed the babies in a sideshow at Coney Island starting in 1903, and charged onlookers twenty-five cents apiece to come in and view the babies and the technology keeping them alive. Similar sideshows were set up in Europe as parts of fairs and expositions, including the 1933 New York World’s Fair and the 1939 Chicago World’s Fair. Although the practice of displaying premature infants for money is certainly morally questionable, it helped pave the way for modern neonatal intensive care. Dr. Couney died in 1950, shortly after American hospitals began to use incubators to care for premature babies. Formation of the Modern NICU (1950s-1970s)Doctors and scientists began writing on the care of premature and sickly newborns as early as the seventeenth century; however, it was not until 300 years later that these babies began to receive special care in hospitals. Until the mid-twentieth century, most of these children were sent home without medical intervention; occasionally, they would have a nurse come home with them. It was not until after World War II that hospitals began to create Special Care Baby Units, the precursors to modern NICUs. The creation of special care units for infants was sparked by the realization that heat, humidity and a steady supply of oxygen could increase the survival rates of sickly babies, meaning that hospitals could intervene to help babies live as opposed to just sending them home. Hospitals were initially reluctant to adopt incubators because of their cost, the fact that they limited access to the infants, and the lack of evidence of their effectiveness. Dr. Couney’s exhibitions brought awareness to the effectiveness of the incubator, which encouraged hospitals to adopt the technology. This was further encouraged by the invention of the Hess Incubator by Dr. Julian Hess at the Reese Hospital in Chicago; in addition to providing heat and humidity for babies, the Hess Incubator delivered oxygen to the infants. The following decade, incubators with clear plastic walls were introduced, allowing doctors and nurses to easily see and access the babies. At this time, doctors were beginning to fully realize the danger that infection posed to newborns, especially premature babies. However, the way infection spread was severely misunderstood; it was thought that the biggest risk to a baby was another baby in the nursery. No one thought that a baby could get sick from a healthy adult. Dr. Louis Gluck was instrumental in proving this line of thought wrong. Along with Sumner Yaffe, Norman Kretchmer and Harold Simon, Gluck performed a series of experiments that involved two sets of babies; one washed daily, the other ones not. They would take cultures from both sets and compare them, and it became evident very quickly that the washed babies had fewer pathogens. To show that the children had a low risk of catching diseases from each other, Gluck began keeping the washed and unwashed children in the same nursery- at the time, keeping more than one premature infant in one room was considered a risky idea. This study included about 25,000 babies, and was never completed- the difference in the health between the two groups became so apparent that nurses began washing all of the babies regularly. It was shown that regardless of nursery mates, a baby who was washed regularly was much less likely to become ill than one who wasn’t; according to Gluck, there was “an 8 to 1 difference in acquisition of staph anyplace”. Gluck observed that the biggest issues was getting visitors and staff to wash their hands; to this day, this remains one of the biggest threats in the NICU. After his research convinced him that infections were more likely to be caused by poor hand hygiene than by other infants, Gluck redesigned the special care nursery, and encouraged the use of isolettes and incubators all in one room as opposed to keeping babies sectioned off in isolated cubicles. This allowed doctors, nurses and other caretakers to easily access and tend to the babies. Gluck additionally designed the L/S ratio test, which determined the maturity of infant’s lungs and therefore their chances of developing certain respiratory diseases. Because of these accomplishments, Gluck is often hailed as the father of neonatology. The Contemporary NICU and Family Involvement  Up until the 1970s, there was a very heavy emphasis on using machines to help at-risk neonates and very little on the involvement of the family. However, this began to change in the 70s. The Newborn Individualized Developmental Care and Assessment Program was developed by Heidelise Als, which encouraged family involvement and individualized plans for each baby. The program reduced the number of ventilator days required for children and improved the outcomes of graduates. In this same decade, fathers obtained “nonvisitor” status in the NICU, allowing them to stay with their children outside of normal visiting hours and increasing a father’s role in caring for his baby. The importance of the bond between mothers and babies was understood and maternal-infant bonding was also encouraged at this point. This became even more heavily emphasized in the next decade with the advent of kangaroo care- skin to skin contact between mother and child to promote bonding, stabilize the baby’s breathing, heart rate and body temperature, and help the baby gain weight and grow. Kangaroo care is now encouraged for all parents, regardless of sex. Parental rooming-in- allowing parents to spend the night in the same room as their child- also was established in the 1980s, and older siblings became more involved in the care of babies; at this point, many hospitals established visiting policies for siblings. This allowed the whole family to help care for the baby and reduced the need for parents to look for childcare for their older children. Other family-centered resources were also established, such as support groups and antepartum consultations, helping families connect with other families who understand their struggles and helping prepare families for the difficulty of having a child in the NICU in the case of an at-risk pregnancy. In the 1990s, the increase of technology to care for premature infants as well as an increase in professional knowledge about premature infants gave hope to babies who in previous decades may have been considered lost causes. Babies as young as twenty three weeks gestational age and as small as 500 grams- were successfully treated. Improvements in nutrition management and new technology allowing for precise fluid delivery, the maintenance of temperature and proper ventilation management all contributed to helping these very small infants survive. Care has continued to improve, and the survival rate for babies born at twenty-three weeks gestational age is now at 33%; babies born at twenty-four weeks have a survival rate of about 65%. Survival without any major health complications has also increased. These increases show hope for premature babies and their parents, and trends indicate that survival rates will rise even more in coming years. With increasing technology and awareness, survival for premature and sick infants is slowly turning from an exception into the standard.  References
"Babies On Display: When A Hospital Couldn't Save Them, A Sideshow Did." NPR. Accessed August 13, 2015. Gluck, Louis. Interview by Gartner, Lawrence. February 21, 1997 http://www.nytimes.com/1997/12/15/us/louis-gluck-73-pediatrician-who-advanced-neonatal-care.html Horn, Lucille. Interview by StoryCorps. Fountain, Henry. "Louis Gluck, 73, Pediatrician Who Advanced Neonatal Care." The New York Times, December 15, 1997, Obituary sec. Accessed August 12, 2015. http://www.nytimes.com/1997/12/15/us/louis-gluck-73-pediatrician-who-advanced-neonatal-care.html. Jorgensen, Anne M. "Born in the USA- the History of Neonatology in the United States: A Century of Caring." Accessed August 13, 2015. http://static.abbottnutrition.com/cms-prod/anhi.org/img/Nurse Currents NICU History June 2010.pdf. Pearson, C. (2015, September 8). Survival Rates For Micro Preemies Continue To Improve. Accessed September 9, 2015. http://www.huffingtonpost.com/entry/survival-rates-for-micro-premies-continue-to-improve_55eed4fce4b093be51bbf26c Yaffe, Sumner, Lawrence Adams, Duane Alexander, L. Joeseph Butterfield, Louis Gluck, George Little, Mildred Stahlman, Mitzi Duxbury, Carol Gartner, Lawrence Gartner, and Philip Sunshine. "Neonatal Intensive Care: A History of Excellence." Www.neonatology.org. October 7, 1985. Accessed September 3, 2015.  If you’re reading this blog, chances are your child was born prematurely. This article specifically deals with preemies that were not only born prematurely, but also continue to receive their nutrition by means of a feeding tube. As a first message I would like to say that it is neither your fault that your child has a feeding tube nor has anything gone wrong in the treatment and taking care of your baby. However, the focus and attention of all the care offered has not been specifically directed at transitioning to oral feeds. We will be talking about why this would be an important step if the medical necessity for the tube has ceased to exist, how this can and should be organized, how you can help your infant catch up with it’s delayed or suppressed eating development and also how it can catch up to its current general developmental level without any medical risk. When preterm babies should learn to eat without a feeding tube Any infant born prematurely between the 23rd and 32nd gestational weeks should be discharged home from the neonatal intensive care unit (NICU) or the aftercare unit as an orally eating baby unless major ongoing medical complications require the feeding tube to stay in place for the time being. For preemies whose tube is no longer necessary to be able to successfully transition from tube to oral feeding, parents (under the guidance of their medical team) and the medical team themself will need to encourage oral function already on a non-nutritive level long before the infant is ready to accept any substantial oral feeding. If all goes well the whole transitioning process to full oral feeding should be completed at around the 34th gestational week. At this point the baby will probably weigh around 4.5-5.5 lbs. Latest, the preemie should be eating by the time of the formerly calculated term birthday. Medical studies have clearly shown that there are significant benefits to oral stimulation by finger or pacifier in preterm babies and that it is desirable to achieve oral feeding as soon as possible. Which doctors are capable of releasing preterm babies without a feeding tube As for instance in all institutions focused around the issues of self-regulation and sensitive individualized care, as is the case in most clinical centers following the guidelines and the recommendations of the NIDCAP® (neonatal individual developmental care assessment program), the ambition is explicitly to not discharge any infants - including preemies - on tube feeds. This goal is realistic and can be met by helping all preemies learn to suck and swallow in a self-regulated and coordinated manner so that they learn how the entire process works. Then, step by step and these children are guided towards being fully self sustaining by mouth and only then will the tube be removed. Why releasing children without a feeding tube matters - The negative side effects of tube feeding The work it takes by parents/doctors to help their child/little patient make this transition is well worth it, as oral fed infants suffer much less from the well known troubling negative side effects of feeding tubes. In a recent study observing the largest population of tube-fed infants ever documented, the parents of 425 tube-fed infants (with both nasogastric (NG) and Percutaneous endoscopic gastrostomy (PEG) tubes) were asked to document their children’s reactions to their feeding tube. Nearly all of these children had been tube-fed since birth. The study showed that over 56% of these tube-fed children fight with gagging and retching episodes daily and 50% vomit frequently. As expected, depending on which tube the children had, their side effects varied. What’s astonishing though is that both tubes (nasogastric (NG) and percutaneous gastrostomy (PEG) tube) come with significant negative side effects and that no significant correlations could be found between age, sex, underlying medical diagnoses, type of feeding tube, feeding schedules (bolus or continuous), and parental and child’s behavior regarding the feeding situation and duration of tube feeding. This means that these side effects are endemic to the tube and unless the tube is removed, they will remain! This is a serious problem, especially since f.e. frequent vomiting can lead to malnutrition. Recent statistics in this field show that more than 33% of all tube fed children aged 0-12 months are malnourished as defined by the criteria of the World Health Organization (WHO). The fact of avoiding these typical tube related symptoms by early tube weaning in itself also sets lots of developmental energy free which the infant will then be able to invest into its general and motor development. Now, what are some of the reasons why transitioning to oral feeds can be difficult or seem nearly impossible for your baby? As a medical doctor, I’ve spent more than 30 years of my professional career working in and with NICU’s around the world. Examining and observing thousands of pre-term babies and their first attempts at eating, these are some of the most common challenges I’ve seen them struggle with:
Guidelines for what to do with a tube-fed preemie Given that all of these challenges exist and are present in one child or another, it is very hard to give general recommendations. However, there are some guidelines which make sense for almost any situation where a preemie baby has been born and is fed with a feeding tube. Elements to follow:
Find out if your medical team specifically wishes the tube feeding to be continued or gives your baby permission to transition to oral feeding. If you receive permission, start thinking about which medical organization you want to do the tube weaning with. Please, from the bottom of my heart, don’t try this alone on your own, it is potentially life-threatening for your child if you don’t know what you’re doing. Since you’re not the first to go through this, I’ve asked a mother of a formerly tube-fed preemie to share with me how she went about choosing a medical partner for tube weaning her preemie. You can find her guide here. Having helped wean hundreds of preemies from their feeding tube with my multi-disciplinary team at NoTube.com, these are some of the lessons I’ve learnt. Preemies are fighters and extremely tough. They’ve gone through so much to get to where they are and they will continue fighting! When challenged to learn how to eat orally by an experienced medical team advising parents what to do, preemies are well able to transit to oral feeding from and be fully orally sustaining by the 34th week or, in some cases, slightly earlier. During the tube weaning phase, a period of 2-4 weeks of slowed down weight development is normal and must be accepted. But it’s important to know that the task of tube weaning in prematurely born infants can only be achieved by intensive cooperation and trust between the nurses, doctors and parents! I truly hope this article was helpful to you and would be glad to answer any comments here or to get in touch with me directly, just send me a message here! Written by Marguerite Dunitz-Scheer, MD of notube.
 When you hear someone mention the acronym NICU, what words come to mind? Miracles? Sorrow? Triumph? Struggle? Heartbreak? Hope? Six years ago I heard the torturous sound of an EKG flatline, as my son died surrounded by his family. As is with my love, an ache in my heart still endures. And there are moments when I think of that NICU - the isolette, the tubes, the wires, and my tiny 5 pound baby and I still hear that sound. The sound that many...too many...parents hear every year. But because, his heart stopped beating in the NICU, it is a place I will always hold sacred. His lifetime. Our lifetime together. Every memory, every dream, every hope I ever had, is housed in the NICU. Here are five reasons why I still believe hope lives in the NICU: 1. Big things happen in the NICU Dreams, both new and old, are achieved in the NICU. Every day, babies defy the odds, grow, and learn to thrive. 2. Your home away from home The saying "home is where your heart is" truly applies. In the NICU, the word "family" is redefined. A community thrives here. Parents and medical professionals alike find new love, passions, and friendship. 3. Some of life's most treasured memories will be made in the NICU Ask any parent of a baby that has spent time in the NICU, the NICU is a place where memories that last a lifetime are made. 4. Heroes don't wear capes Heroism comes in many forms in the NICU- in the persistence and dedication of it's staff; in the spirit of the tiniest of patients; and in the unwavering love parents have for their children. 5. A place with a vital purpose The NICU provides thousands of babies every year with the best chance at life, when those first moments in the world are the hardest.  The NICU will forever remain my son's only home. The place of his first's and last's. The space where every memory lives, including every kiss and every sweet embrace. Our brief time in the NICU profoundly changed the course of my life - my career, my relationships, my philanthropic interests. More importantly, it showed me how love and hope endure, even in our darkest of hours. Because he lived, the NICU will forever be a home for my hopes. Written by Sarah King, President for Project Sweet Peas
 Dear Preemie Parent, Hi there! I saw you today. I smiled. Maybe I asked you how old your preemie was or maybe I didn't. I feel like I can sometimes pick a preemie out of a crowd. One day, you might too. I want to tell you a little bit about about hope. It took me a while to get here. Sometimes I thought about it every day – about when we we'd get “out of the woods” and no longer have fear that there would be something else wrong with our preemie. I have spoken with many preemie parents over the years. One common thing that almost all parents remember is what the doctors told them about the future in those first days. I too remember. Do you? My preemie was born with no heartbeat and was not breathing. What we were told is a) he probably wouldn't survive. There was a neurologist that came to my hospital room the day after our son was born. (Thank goodness I was still hopped-up on morphine at the time that even though I heard those words, they didn't process in my brain. I am pretty sure that was my body's defense mechanism). And, b) if he did survive we needed to be prepared for a long road of having a child with severe brain damage. Today, my preemie is an amazing student – a far cry from what the doctors told us almost 12 years ago. He plays sports – wrestling, baseball, basketball and football. I try not to think about it too much, about how far we have come – how far he has come, but when I do, I am in awe. I don't think about the fact that I had to call my husband from our son's bedside and tell him he needed to come to the hospital because our baby might die that day. That thought will be tucked way back in the depths of my brain forever, I am sure. I don't think about the fact that I was paralyzed with fear in those 3 months we spent in the NICU. I cried almost every day – more than once. Did you? I was angry, sad, scared and happy all in the same thought. Were you? Listen with your “third ear” to the doctors. Doctors are amazing, intelligent individuals and I wouldn't want their job, not at all. 99% of the doctors we have come in contact with over the last 11 ½ years have been awesome. But what one doctor told me is that sometimes they are just really good guessers. Of course, too, we had one doctor in the NICU that even though they knew that there was a real possibility of a grim future, he gave us the ability to hope for something more. Dr. S will always hold a special place in our hearts. He was the only one who gave us the tiniest bit of information to think that we'd actually make it outside the NICU doors with our baby (alive and well!). When we go back and see the doctors that saw him in those early days, they are amazed and impressed in the young man has become. Our story is unique – or is it? I have heard so many “we thought he'd never make it” stories over the years and I love every single one of them. One of the residents told me while we were still in the hospital that in the middle of the night, when she had to stay overnight in the hospital, she would come into the NICU and hold our little guy. She said she knew she was holding a miracle and that nobody she knew had ever seen a baby survive who started out the way he did. So, doctors go on what they know. My son's doctors only told us what they had seen. How I wish I could remember the name of that neurologist - I'd love to show him how far we've come. But, I want the doctors, to give another parent a little bit of hope. Maybe they can tell the next set of parents who have a baby who has an APGAR of 1, is barely breathing and may not survive - maybe they will tell them that while their little fighter has had a rough start and a lot of babies don't do well after this, there are some babies who pull through and surprise the hell out of us. I hope to God that your baby is one of those babies. Meanwhile, we are going to do everything we can to make sure that he is. We're going to try and we hope you come back and show us in 11 years how great he's doing. And then those parents are going to think to the future. 11 years from now!? Wow. They are going to try to picture their life with a 11 year old. Sass and eye rolling and a stinky boy coming home after practice (and he will offend you with how much little boy sweat smells) and they will smile through their tears, because someone gave them a little bit of hope. Are you that parent? Have hope. Don't listen to all the doom and gloom. Pray if you're the praying type, ask the universe to help you get through your bad days if that's what it takes. But, please, oh please don't loose hope. I've been there. We've all been there (did you know we're a part of an exclusive club?). Ask for help when you need it. Find organizations like ours that will link you with a mentor who has walked in similar shoes. We get it. Accept our hug – in person or virtual. Love, Another Preemie Mom who gets it  Beth is the President of The Little Bear Foundation. She is the mom of 3 children - one preemie and two full termers. When she is not helping others through her Little Bear work, you can find her on the sidelines of a football field, basketball court, baseball field or soccer field cheering on her amazing kids.
 Our story begins when I found out in April of 2014 that we were expecting again. My husband and I had 4 children already and we could not wait to meet our new blessing! We went for our 2nd prenatal appointment and found out we were pregnant with twins. Four weeks later, we found out that they were identical twin girls who were suffering from Twin to Twin Transfusion Syndrome (TTTS) at 16 weeks. From then on I was on bed rest. The following week we drove to Cincinnati for the Placenta Abrasion surgery. After seeing 4 different specialists and four hours of surgery, we were in recovery. That night, we woke up to check on the girls, who we had already named Isabella Grace and Lillian Mae Autry, to find out twin B, the "donor twin" (Lilly), didn't make it through the night after surgery. We came home and for 4 weeks I was on bedrest. I woke up one morning at just 20 weeks to find my water had broken. I went to the hospital for a 3 day stay for antibiotics and to measure fluids. I was discharged and sent home with them saying we will check fluid each week and go from there. If she was still thriving at 24 weeks, I would be hospitalized for the remainder of the pregnancy. Finally after the longest 4 weeks of my life, I was admitted. Isabella (Ella), twin A, was fighting hard!!  After almost 6 weeks in the hospital on bed rest, I had a placental abruption, which meant I needed an emergency C-section. We had no idea what was going to happen with Ella. She came August 19th 2014, and took her first breath by herself, which didn't surprise any of us as hard as she fought to be in the world! Then they vented her and rushed her away. I went to recovery for an hour, and then was rushed to the NICU, while being told, "they had done everything they could do." I asked, "Is her heart still beating?" They replied, "yes." ..and I said, "keep trying!" I knew we did not go through all that for her not to live. Family and friends started praying all over the U.S. Her heart kept beating. She made it through the night. The next day still told they didn't think she would make it. But, she kept fighting. We were allowed to touch her. We were encouraged to spend as much time as possible with her. Finally that afternoon on the 2nd day, while we were touching her, her vitals began to signs of improvement. The next day, we found our she had a brain bleed in two sections of her brain. She needed tubes in her lungs and her vitals were up and down. They said her future was unknown. She could be disabled, delayed, who knew. We just took it one day at a time and the NICU roller coaster began!  There were ups and downs. She stayed 104 days with the amazing staff that we left a piece of heart with each night! We brought her home December 1st 2014. Many specialists still see her, and therapists still work on her. But now, she just turned one. Her Hydrocephalus, that she was diagnosed with, is "maintained without surgery." The hole in her heart has healed. She's still on oxygen at night. She crawled in therapy this week. She's a healthy, smart, sassy little girl that brightens the world of every one that meets her. And last week when we went for her check up, they took the "developmental delay" off her chart. Our girl has "caught up!" She's a miracle and we have been so blessed.  A special thank you to the Autry's for sharing their story.
 A wife that loses a husband is called a widow. A husband that loses a wife is called a widower. A child that loses its parents is called an orphan. There is no word for a parent that loses a child. That’s how awful it is. I can think of a few words to describe losing a child: devastating, broken, empty, crushed – but these words don’t even sum it up in totality. There is no one single word in the English language that can truly encompass a loss of such magnitude. I lost my daughter, Nevaeh nine years ago. She was born 10 weeks early with several complications. She passed away in the NICU six weeks later. Her death left a void in me that can never be repaired. It left an emptiness that never goes away. There were days I felt like I was going to drown in the darkness of grief. But eventually, I floated to the top. I am a grief survivor. As with grief and loss in the case of the death of a loved one, NICU parents are often expected not to speak of their grief. Death is hard to talk about no matter what, but it makes it even harder when a baby is involved. I found most people very uncomfortable when I brought up my daughter. They didn’t know what to say. A lot of people didn’t dare ask me about her life, or how I was coping after she died. I think they were afraid to bring the subject up, in fear of stirring up emotions. What they didn’t realize is that the emotions were already there no matter what. I wanted to talk about my daughter. I was so afraid that if I didn’t, she would be forgotten. I wanted people to know she had existed, that her life here on Earth – no matter how brief – mattered. I wanted people to acknowledge I was a mom – even if I didn’t have a baby to show for it. I’d meet people and they would ask if I had any children. Do you know how awful it is to have to sit and pause and think about how to answer that question? Because if you answer it truthfully, that yes – you have one daughter, but she is in Heaven now – people get uncomfortable and don’t know how to react. But if you simply say no – you feel like crap because you feel like your not acknowledging your child. Just when I thought I was getting a handle on grief, my daughter’s first birthday approached, and I was filled with vivid memories of her birth and short life. It brought all the feelings of loss, anxiety, panic and devastation all over again. Nine years later, I still cry on her birthday and the date of her death. I think some people still have a hard time understanding the emotions that her birthday and day she died brings. Grief is an awful thing. It is so hard to understand, and part of the reason is we all grieve differently. There are the five stages of grief: denial, anger, bargaining, depression and acceptance. I went through every one of them. I like to sum up grief like this: Grief is like getting a bad cut on your arm. At first the cut is really bad and deep and raw. But after time, it starts to heal. It never really goes away, and your arm is never really ever the same. And sometimes you look down at your arm, and see the scar, and the memories of how you got it flood back. That is grief in a nutshell. It does get better, but it never goes away. I know that I will never be the same, I am forever changed. I am a grief survivor. 
 When we found out I was expecting triplets, the doctors quickly made us aware that it was a high risk pregnancy and that the babies would likely have to spend time in the NICU. I tried to prepare myself for the NICU experience, but I could never fully understand what a parent in the NICU goes through until I went through it myself. Our baby A (Savannah) was in the NICU for 6 days before we lost her. Our baby B (Paige) spent 55 days in the NICU before coming home and our baby C (Emma) spent 34 days in the NICU before coming home. The first time I saw my girls, I was overwhelmed because they were hooked up to so many machines. I went through so many emotions during our NICU stay that it was like being on a rollercoaster most days. Here are some of the emotions parents may experience during their time in the NICU: Fear: As a parent you want to protect and shelter your baby, and you can’t when your baby is in the NICU. You might not fully understand what’s going on and fear that your child may have a serious illness, a disability, or even die. The NICU is a scary place. Anxiety: The NICU goes hand-in-hand with anxiety for many parents. I remember being worried that my phone would ring at any time with bad news from the hospital. I was worried that I wouldn’t hear my phone and then I wouldn’t be there for my girls. Every time I called the nurses to check on our babies, I held my breath until they said everything was going well. Anger: Many parents feel anger that they didn’t get the birthing experience they hoped for, that they can’t take their child home right away like other parents do, that they can’t help their child, and that they can’t control events that happen in the NICU. You may even find that you’re angry at yourself. You may be angry that your body couldn’t protect your baby or that you couldn’t carry your baby longer. You may feel angry at other people as well and feel like they just don’t understand what you’re going though. I often felt angry that not only did I have trouble conceiving children, but I didn’t get the birthing experience that I’d always imagined and then we lost one of our babies. Guilt: You may also feel guilty and wonder what you did wrong or what you could’ve done differently. I often found myself asking “what if” and “why me.” It took me a long time to sort through my guilt, especially after we lost Savannah, and it still resurfaces. I work hard to acknowledge these feelings and to know that I did everything that I could for my girls. Loss: When you find out you’re pregnant, you have expectations of what things will be like when you have your child. Most parents picture a healthy, full-term child who they will get to take home after a few days. You may mourn the loss of this experience. Many mothers of premature babies also find that they miss feeling their baby inside and mourn the end of their pregnancy. Joy/pride: There are some good emotions that you experience in the NICU as well. You may experience a sense of joy as your baby starts to make progress. You may feel proud of your child as he overcomes obstacle after obstacle and has many of his firsts (first bath, first bottle, first smile etc.). Here are some helpful coping strategies to help you deal with the ups and downs of being in the NICU: Celebrate small steps!! Your child is fighting big battles and every triumph, no matter how small, should be celebrated! Take time for yourself. You may feel like you need to be at the NICU all the time, but you’ll burn yourself out if you don’t take breaks. Take this time to do something you enjoy or do something with your partner to reconnect. Start a journal. Writing in a journal during your NICU stay can help you keep things in perspective on those really rough days. Talk to supportive people. The NICU can be a lonely place, so work to find people to connect with who have similar experiences (even if it’s just an online support group). I don’t know how I would’ve made it through my pregnancy or NICU stay without my triplet moms support group. Allow yourself to cry if you need to. Help with the cares for your child. Change diapers, help give baths, take temperatures, and ask lots of questions. Getting involved in everyday care helps you feel more connected. Remember to be gentle with yourself. Having a child in the NICU is overwhelming and trying. You’re doing the best you can do. Try to remember that one day soon, the NICU will be a distant memory.  Shelly Hopkins is a Project Coordinator for Project Sweet Peas division Savannah's Snowdrops.
 Towards the end of pregnancy, thoughts are preoccupied with delivery. Will it hurt? What pain relief will I need? Even, how will I know that labor has started? I found myself asking. But, not once did it cross my mind that my baby might be poorly. On the tenth day past my due date I lost a little fluid. I had planned on having my baby at a midwife-led unit, as I was considered low risk, so I went in and they confirmed that it was in fact amniotic fluid. I was sent home and told to keep checking my temperature and rest up until contractions started. I had a few contractions on and off over night. In the morning I went back and as labor had not progressed I was sent to the hospital. Poor CTGs and a LOT of meconium present when my waters were broke meant they wanted me in theatre for an emergency section, and fast. Penelope arrived half an hour later. The room was full of people but I couldn't help but think that it seemed dreadfully silent. We hadn't heard her cry. I, however, had begun to cry and it was as I looked at my husband that we heard the faintest of whimpers. I caught a glimpse of her as she was wheeled out. She needed help breathing. Whilst I was in recovery my husband had been to see her in NICU and brought me a picture. She was perfect. But, it wasn't looking good, she was on 100% oxygen and couldn't breathe on her own. She had severe meconium aspiration and persistent pulmonary hypertension as a result. I managed to get myself into a wheelchair and go and see her. By this point she was on an oscillator, which was just petrifying to behold. My brand new, delicate baby was shaking away. We sat there for hours watching her sats, they were going down instead of up. Nitric oxide didn't work either. We sat with her for ten hours and then the doctor wanted to speak to us. They had exhausted all the options at our local NICU, there was nothing more they could do now. He mentioned something called ECMO but there are only a few places in the country that do it. The closest place to us was Glenfield, Leicester, three and a half hours away. Luckily for us, there was a bed and Penelope met all the criteria to qualify for it. ECMO is basically a lung bypass. Blood is taken out of the heart by a tube in the neck and the oxygen is added to it outside of the body and then the blood is returned, doing the lungs jobs, allowing the meconium to be cleared out. The team from Leicester came the following day, put her on ECMO and took her to Leicester in an ambulance where she stayed on ECMO for 36 hours. My husband followed her there and I was discharged the following day and met them both there, and although phenomenal to behold, it was easily the most terrifying thing I have ever witnessed in my life. She was then brought back to our local NICU in a helicopter! And, yes, they had teeny tiny ear defenders for a newborn! She was already proving to be a fighter. She was off the ventilator 24 hours later, but our NICU journey was nowhere near it's end. She was now breathing on her own but was unable to maintain a safe blood sugar level without a high concentration of dextrose. It took a couple of weeks to get the results back from the myriad of tests performed. It transpired to be something quite rare we were dealing with. She has congenital hyperinsulinism which means that she produces too much insulin, like the opposite of diabetes, causing dangerously low blood sugar. This was completely unrelated to her breathing difficulties she initially faced. Even though she was admitted to NICU with what was a relatively "common" newborn problem for full term babies, that being meconium aspiration (albeit she had it to the extreme, the most severe case our local NICU had seen) it was dealing with awaiting a diagnosis for something more complicated afterwards that was particularly difficult. I can certainly sympathise with any parent whose child is in NICU with a rare, genetic condition not picked up on during pregnancy and waiting for the results of test after test. And, perhaps the most wearying thing of all was not knowing when we would be able to bring our baby home.  Once she was on her medication and beginning to stabilize there was light at the end of the tunnel. However, from there we had difficulty "teaching" her how to feed as she had previously been NGT fed whilst we awaited a diagnosis. This was what felt like the most tedious part of our stay in NICU. She had reflux and consequently ended up on even more medications and with a speech and language therapist and dietitian visiting her now. It seemed that she could not keep a bottle down, even the tiny bit she could manage. And, worse, when she was sick she would go hypo and her blood sugars would drop. This prolonged our stay in NICU a few times. But, after six weeks and two days and a very long discharge planning meeting and two nights 'rooming in' with Penelope, we were able to take her home. With the NGT still in. My husband was shown how to pass one. She was off it in no time when we brought her home and could practice feeds round the clock! I think that even though it is a great shock delivering a baby prematurely, it is just as much of an unpleasant surprise having a poorly full term baby that needs neonatal intensive care. What I would like to let any parents in a similar situation know should they be reading this, is that it really does get easier. And once you can accept that taking your baby home will happen when they are ready, it can even become enjoyable! The nurses are utterly fabulous, what a job to do! And are of great comfort. We documented and enjoyed some of Penelope's "firsts" while we were there as if we were at home, but had the advantage of a helping hand. For example, the first bath! It is a place full of ups and downs, but take solace where you can, even if it is reading this for five minutes while your new baby takes a nap. And, most of all CONGRATULATIONS on your new arrival, from a parent of a 'NICU grad'. Gianna Pickup   Gastroschisis, the what.....
Gastroschisis is a birth defect that causes the intestines to protrude from a hole in the abdomen, typically to the right of the umbilical cord. Occasionally, other organs are involved as well. This must be repaired surgically after birth, although surgery is not always possible immediately and depends on many factors including the amount of bowel outside of the body. While approximately 90% of affected infants survive in industrialized nations with proper medical care, there is still a 10% mortality rate due to complications or related defects and infections – even with the best medical care. [In the USA, published survival rates range from 83%-97%1]In nations without access to proper medical care, the mortality rate is often 100%. In the United States, Gastroschisis affects 1 out of every 2229 babies according to the CDC2, although the actual rate varies by state. California, for example, published a 2005 report which showed the incidence to be 1 in 1727 births3and Texas rates show the incidence to be 1 in 1683 in 20094. In Canada, the current rate is 1 in 2272 with an exception of the area of Nunavut, which for unknown reasons is as high as 1 in 510 births5. Worldwide, rates of gastroschisis in industrial nations vary between 1 in 2000 and 1 in 33336, although some regions have higher rates, such as Wales which is reported at 1 in 16127 births and an area in Australia with an incidence as high as 1 in 8928. According to the International Clearinghouse for Birth Defects Surveillance and Research, a 2009 report from 16 separate registries shows that South America as a whole has the highest reported incidences of gastroschisis in the world, at 1 in 1063 births4. It is worth noting that there is little to no data collected on incidences in Africa. Rates of gastroschisis are increasing worldwide, and this trend is being called a “pandemic” by many researchers9. The medical community still does not know what causes gastroschisis, but researchers have found many correlations and risk factors including aspirin and other medication use10, exposure to certain chemicals, low maternal body mass index, and genitourinary infections11. Studies from Utah are demonstrating a familial link to gastroschisis, with one study showing that 23% of families studied had more than one relative with gastroschisis12. However, the single largest risk factor for having a child with gastroschisis continues to be young maternal age. The CDC continues to monitor these trends in the US13. Additionally, a 2006 study from the UK showed that mothers under 20 years old have an incidence of gastroschisis ranging from 1 in 1123 to 1 in 40914. Although the overall prognosis is good for most infants born with this birth defect provided they have access to medical care, complications do arise. Studies show that gastroschisis is the leading cause of intestinal transplantation15, and that 40% of gastroschisis survivors will need to be readmitted to the hospital at some point due to complications, the most common of which are bowel obstruction and abdominal pain16. Furthermore, having a child with a birth defect can put many stressors on a family that others simply do not experience, and it is recommended that families have a strong support network17. The Why of Avery's Angels: Avery’s Angels Gastroschisis Foundation is the only nonprofit in the United States to assist and support those affected by gastroschisis. When we first formed, Avery’s Angels was the only nonprofit in the world with this cause; now we are joined by the Luey Jacob Sharp Foundation18 in the United Kingdom. In 2008, Avery's Angels founder, Meghan Hall and her partner Jared Rauen found out that their little boy would be born with gastroschisis. During Avery’s life, he not only provided them with hope and joy, there was an incredible rise in their community to support the little family through the process. From meals, to gas cards, prayers and thoughts to folks donating blood in solidarity for Avery’s fight. Even Avery’s team at UNC Chapel Hill NCCC was also heavily involved in educating and supporting Meghan and Jared during Avery’s time. There were angels around them the entire time. Avery stayed 107 days in the NICU- from April 14th 2009 and passed on July 30th 2009 unexpectedly from unforeseen complications. During this time the little family had many happy memories and a well-supported experience because of the tremendous efforts of their entire community. At the time there was not a centralized organization for support or information. Inspired by the “angels” that had been present in their own experience and fueled by the hope that was Avery’s life, Meghan began blogging about forming a foundation to promote that community of support, education and awareness for others affected- providing the same angels they had, for others. With the encouragement of “Avery’s Angels” the team at UNC Chapel Hill, their family and community, Meghan launched Avery’s Angels September of 2009. Between Meghan’s first blog post and Avery’s ngels acceptance as a registered 501c3 nonprofit on April 29, 2011, some amazing individuals came together and worked collaboratively to make the dream of a gastroschisis nonprofit possible. The initial core team was Meghan Hall, Herb Richter, June McDowall, Sheila Palus, and Kayte Thomas. The core team worked hard on planning, advocacy, legal work, and logistics to make the foundation possible. Added in soon after were Lea Krutel, Megan Turcotte, and Autumn Hernandez who further contributed to the founding efforts. These passionate pioneers were all impacted by having a child in their family born with gastroschisis – a combination of parents, grandparents, and great grandparents who wanted to make the world a better place for others who were dealing with the same experiences. Each of them brought a unique perspective to the budding organization because of their specific outcome with gastroschisis; they brought with them the knowledge of life, death, short bowel syndrome, divorce, advocacy, heart break, and love beyond measure, amongst other things. It is to this committed group of people that the world owes gratitude for the existence of the first nonprofit in the world dedicated to supporting gastroschisis families. To this day, we are founded on that initial cause of providing support to families as being our primary purpose, funding the needs of the cause above all else, and encouraging research to discover the causes and promote prevention. What do we do? And why do we do it? Avery’s Angels Gastroschisis Foundation’s mission is to promote awareness, research, and support for gastroschisis worldwide. We accomplish this by: – Creating a national and international network of families dealing with gastroschisis and related complications. – Providing emotional and financial support to families who have or are expecting babies born with gastroschisis. – Supporting friends and families of survivors of gastroschisis and those who have lost a loved one to this disease. – Promoting national awareness annually via Gastroschisis Awareness Day events every year on July 30th. – Collaborating with clinicians to facilitate research to find the cause. – Assisting in other ways as indicated by the circumstances. AAGF is an all-volunteer foundation. There are no paid employees. We depend on your donations and volunteers to accomplish this vital mission. Please encourage family and friends to “Get Involved.” To learn more about how you can help visit the Volunteer page on our website! It is tremendously important that our parents and patients have lifetime support, which is what Avery's Angels is founded on providing. The initial NICU stay can range anywhere from 14 days (our personal record!) to over a year. One of our parents, Laura Violet Marie writes on the most important advice for an expecting or NICU gastroschisis parent is: "Patience! It's probably the hardest thing to do but you cant rush those little tummy's.. We all want to go home right away and as each day adds to your total you get more and more anxious and envious of each mom that got to take their baby home the next day.. But your time will come and your baby will heal in the time that he is she is supposed to! Tell people to stop asking you when he/she will be coming home! I was frustrated when people would ask me because i myself didnt know and i follow gastro mom's stories now and see countless people comment on their pictures "when is she coming home? How much longer?" And it aggravates me for them!" This is so true! Gastroschisis is variant, based on many physiological features, how large the defect is, how much intestine was out, how extensive the damage was/is, what gestational age the baby was born at, how the bowel is recovering or functioning. This is why it is crucial that our parents have proper support from those who have been through this and most importantly set up a good line of open communication with their physicians and practitioners. Gastroschisis parent Erin Herrman says: "Most importantly, ask questions. It's scary to leave your new born there alone ( alone because YOU are not there 24/7). The worst feeling is to be alone and confused. Do not worry that your question(s) might sound stupid. There is no such thing as a stupid question. Knowing and understanding everything your newbie is going through will make the time apart more bearable and make you feel more comfortable knowing the best health care professionals are there to treat your baby in a way you may not be incapable of." This is crucial. While it is easy to get caught up with how disenfranchising being a NICU can feel for a parent, it is important to take a breath and find the right way to communicate with those around you. Remember, the physicians and practitioners are there with the same goals as you are- healing, health and home. It is extraordinarily difficult to build a relationship in the NICU especially with so much going on, but speaking up, speaking often and seeking those opportunities will not only benefit your child, it will also help a parent heal from the NICU experience too. Recovering from your NICU experience is important. Especially for our gastroschisis parents. Having confidence in both yourself as a NICU parent and the medical relationships you are forming is crucial. Building those healthy relationships with the team will help families feel more confident at home. Most importantly if and when signs may pop up at home that warrant seeking medical involvement, help families will not have as many reservations for seeking timely professional help. Odd temperature spikes, tummy pains, changes in stools, excessive vomiting, distention in the bowel area can all indicate concerning signs that timely medical intervention can improve outcomes for. Support is everything, so asking for help is the name of the game, Gastroschisis mother Belinda Smithson says: "We didn't receive any help from anyone during our stay or when we arrived home. It was awful and I wasn't going to ask for it. Before you go into hospital write a list, or get others on here to write a list of things that could be of help. We lived on takeaway food for the whole time and it was awful frown emoticon a nice home cooked meal would have been lovely. This goes for when you get home too." But make sure you have a good balance of NICU visitors (remember! more people bedside ups the risk of infection!) once baby gets home it is OK to take your time with visitors if you feel you need alone time (finally!). Gastroschisis mom Sarah Boyer says: "Be sure to make time for you, your husband and child to get things back to normal before inviting any other family members over. Whether this takes a week or a month...they can wait. Of course, if you need help, ask them! But don't feel obligated to have everyone over right away." Support is what our families need, from their practitioners to their families and also in the resources that are available to them. That's where Avery's Angels has found its purpose. We not only provide all the information accessible to our families, we also have over 10 programs to help support our families across the entire NICU experience. We are here to be your angels! Learn more about Avery's Angels at www.averysangels.org Citations:
|
 RSS Feed
RSS Feed